
Hashimoto’s, Fatigue, and the Nutrient Gaps Your Thyroid Panel Is Not Showing You

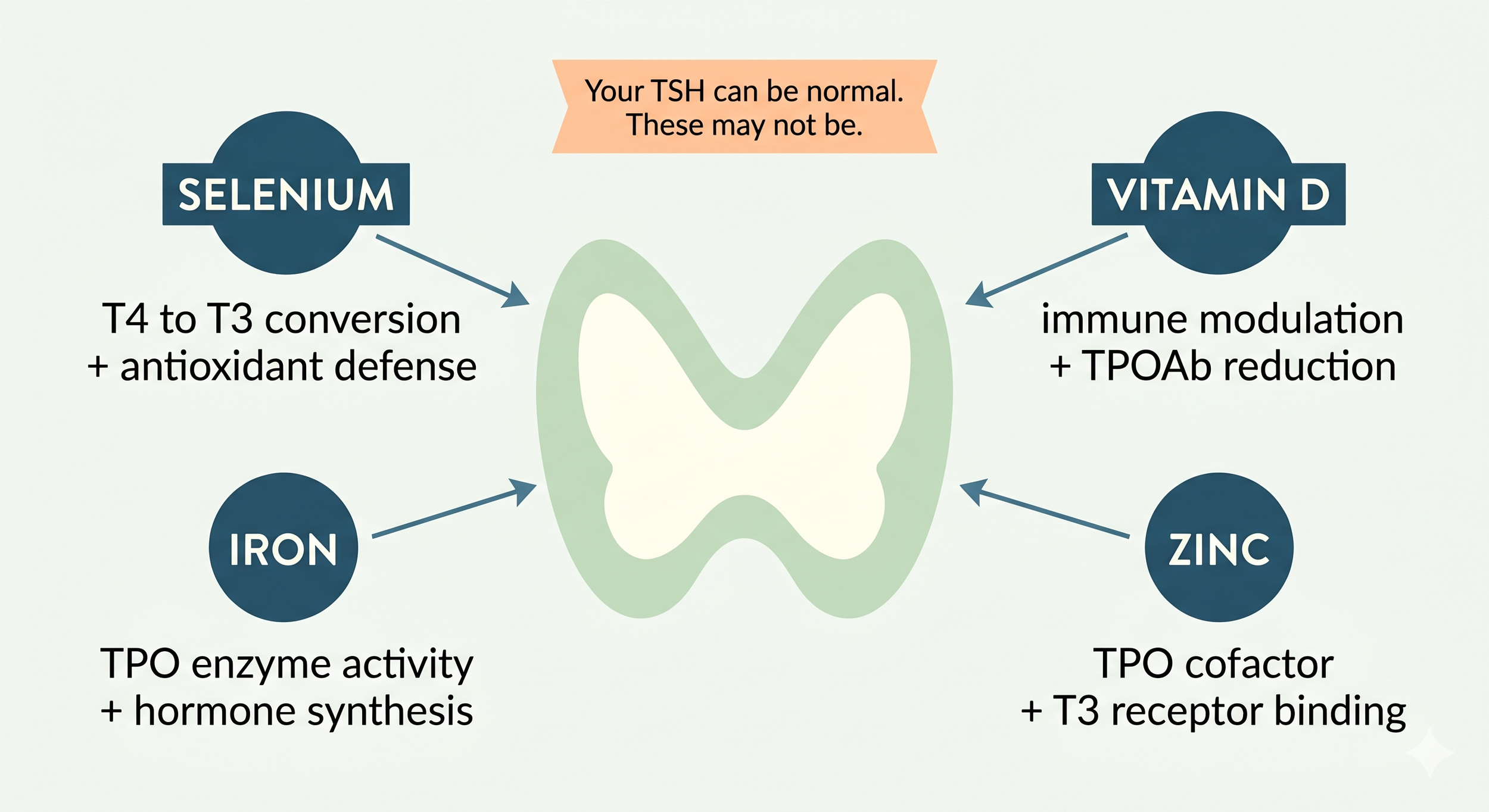
Your TSH came back normal.
Maybe your T4 did too. And yet you are exhausted, your hair is thinning, your brain feels slow, and everything takes more effort than it should.
If you have Hashimoto’s thyroiditis, this is one of the most common and most frustrating experiences. Because a normal-range TSH does not mean your thyroid is working well. And it almost certainly does not mean your nutrient status is adequate.
If you have Hashimoto’s thyroiditis, this is one of the most common and most frustrating experiences. Because a normal-range TSH does not mean your thyroid is working well. And it almost certainly does not mean your nutrient status is adequate.
Hashimoto’s is the most common cause of primary hypothyroidism in iodine-replete areas, with an incidence of 0.3 to 1.5 cases per 1,000 people, affecting women at significantly higher rates than men (Durá-Travé & Gallinas-Victoriano, 2024). What most standard panels miss is the relationship between thyroid function and the specific nutrients your thyroid depends on. This post covers four of the most clinically relevant: selenium, zinc, vitamin D, and ferritin.
Why TSH Is Not the Whole Story
TSH, or thyroid-stimulating hormone, tells you what the pituitary gland is doing in response to thyroid hormone levels in the blood. It is a downstream measure, not a direct measure of thyroid tissue health or hormone conversion.
In Hashimoto’s, the immune system is actively attacking thyroid tissue. The antibody markers of this process, thyroid peroxidase antibodies (TPOAb) and thyroglobulin antibodies (TgAb), can be elevated for years or even decades before TSH shifts outside the reference range. By the time TSH moves, significant tissue damage may have already occurred.
Even when TSH is within range, the conversion of T4 to the active hormone T3 may be impaired. T4 is largely an inactive storage form. T3 is the hormone that actually enters your cells and drives energy production, metabolism, cognition, mood, and temperature regulation. If conversion is poor, TSH can look normal while your cells are running on inadequate T3 (Shulhai et al., 2024).
Several nutrients directly affect deiodinase enzyme activity, which is responsible for that conversion. When those nutrients are low, the conversion problem can persist even in the presence of a normal TSH.

Selenium: The Most Critical Thyroid Mineral You May Not Be Testing
The thyroid gland contains the highest selenium concentration of any organ in the body (Leone de Souza et al., 2025). That is not a coincidence. Selenium is structurally embedded in the enzymes that do some of the most important work in thyroid physiology.
How selenium works in the thyroid
Selenium is an essential component of iodothyronine deiodinase (DIO), the enzyme that converts inactive T4 into active T3. When selenium is deficient, DIO activity is reduced, and the conversion of T4 to T3 decreases. This can result in elevated T4 with inadequate T3, meaning you have the raw material but not the active hormone (Kawai et al., 2018; Shulhai et al., 2024).
Selenium is also an essential component of glutathione peroxidase (GPx), the enzyme that neutralizes the hydrogen peroxide produced during thyroid hormone synthesis. During this synthesis process, the thyroid intentionally generates hydrogen peroxide as part of how it incorporates iodine into thyroglobulin. If GPx activity is low due to selenium deficiency, hydrogen peroxide accumulates, causing oxidative damage to thyroid follicular cells. This oxidative stress is directly implicated in the autoimmune inflammatory process characteristic of Hashimoto’s (Leone de Souza et al., 2025; Shulhai et al., 2024).
What the research shows
A 2025 narrative review published in Archives of Endocrinology and Metabolism summarized the evidence on selenium and thyroid pathophysiology, noting that low selenium levels are associated with increased prevalence of thyroid diseases including hypothyroidism, subclinical hypothyroidism, and autoimmune thyroid diseases. An observational cohort study of 1,254 individuals found an increased incidence of Hashimoto’s thyroiditis after a 6-year follow-up in those with low selenium status, particularly in women (Leone de Souza et al., 2025).
A meta-analysis of 16 trials concluded that selenium supplementation reduced TPOAb levels, especially in patients already on levothyroxine replacement therapy (Shulhai et al., 2024). A more recent meta-analysis found a substantial decrease in TSH levels and anti-TPO antibodies in euthyroid and subclinical hypothyroid individuals with Hashimoto’s who received selenium supplementation without hormone replacement therapy (Shulhai et al., 2024).

A study in patients with severe selenium deficiency found that selenium deficiency was associated with elevated free T4 levels, suggesting impaired T4-to-T3 conversion. When selenium was supplemented, free T4 levels decreased, consistent with restoration of deiodinase activity (Kawai et al., 2018).
The evidence is not conclusive enough to support universal selenium supplementation, and excess selenium can be harmful. Selenium status should be assessed before supplementing. But the research is clear that adequate selenium is essential for thyroid autoimmunity management, and deficiency is a modifiable factor that standard panels routinely miss.
Zinc: Often Overlooked, Clinically Relevant
Zinc plays a multifunctional role in thyroid hormone synthesis, metabolism, and signaling that is underappreciated in standard thyroid management.
How zinc works in the thyroid
Zinc is a required cofactor for thyroid peroxidase (TPO), the enzyme that catalyzes the iodination of thyroglobulin and the coupling of iodotyrosine residues to form T4 and T3. Without adequate zinc, TPO activity is impaired and thyroid hormone synthesis is compromised at the production step (Shulhai et al., 2024).
Zinc is also involved in T4-to-T3 conversion, specifically as a cofactor for type 1 and type 2 deiodinase enzymes. And it plays a role in how thyroid hormones bind to their nuclear receptors in target cells. Zinc deficiency can impair receptor function and reduce the effectiveness of thyroid hormone signaling even when circulating hormone levels appear adequate (Rabbani et al., 2021; Shulhai et al., 2024).
Zinc also has direct antioxidant and anti-inflammatory properties. In the context of Hashimoto’s, where chronic immune activation and oxidative stress are central to disease progression, zinc’s role in reducing reactive oxygen species and modulating T cell differentiation is clinically meaningful (Shulhai et al., 2024).
What the research shows
In a randomized double-blind placebo-controlled trial, 86 patients with hypothyroidism received daily co-supplementation with zinc, magnesium, and vitamin A for 10 weeks. The intervention group showed significant increases in free T4 and reductions in inflammatory markers including hs-CRP, while the placebo group showed worsening of total antioxidant capacity and increased inflammation (Rabbani et al., 2021).

Zinc deficiency has been associated with thyroid enlargement in both children and adults. A study of 68 school-age children found an inverse correlation between zinc concentration and thyroid size. Adults with nodular goiter, particularly in iodine-deficient regions, have also shown lower zinc concentrations (Shulhai et al., 2024).
A 12-week RCT of zinc supplementation in children and adolescents with autoimmune thyroiditis found that while thyroid hormone and antibody levels did not change significantly, levothyroxine dose requirements increased significantly in the placebo group but not in the zinc-supplemented group. This suggests zinc may play a role in supporting the effectiveness of thyroid hormone replacement therapy (Shulhai et al., 2024).
As with selenium, the evidence supports assessing zinc status rather than supplementing without testing. Zinc deficiency is associated with hypothyroidism through multiple mechanisms, and it is one of the more commonly depleted minerals in this population.
Vitamin D: An Immune Modulator with Direct Thyroid Implications
Vitamin D receptors are present on thyroid cells and on virtually every immune cell in the body. This positions vitamin D not just as a bone or calcium hormone but as a central immune regulator, which makes it particularly relevant in autoimmune conditions like Hashimoto’s.
How vitamin D affects thyroid autoimmunity
Active vitamin D exerts its effects through the vitamin D receptor (VDR), which is expressed on T cells, B cells, dendritic cells, macrophages, and neutrophils. Through the VDR, vitamin D inhibits the production of pro-inflammatory cytokines including IL-6, IL-8, IL-12, IL-1, and interferon-gamma, while increasing anti-inflammatory cytokines including IL-10 and IL-4. It also suppresses dendritic cell maturation and reduces excessive adaptive immune activation (Durá-Travé & Gallinas-Victoriano, 2024).

In Hashimoto’s, which is a T-cell-mediated autoimmune disorder characterized by lymphocytic infiltration of the thyroid, this immunomodulatory function of vitamin D is directly relevant. Low vitamin D may reduce immune tolerance and allow the autoimmune process to proceed more aggressively. Vitamin D also prevents excessive T-cell activation, inhibits Th17 cell development, and promotes the differentiation of regulatory T-cells (Tregs), which are central to immune tolerance (Lebiedziński & Lisowska, 2023).
What the research shows
There is extensive evidence that vitamin D levels are significantly lower in patients with Hashimoto’s compared to healthy controls. A 2024 narrative review summarizing the literature from 2011 to 2023 confirmed a consistent inverse relationship between serum 25-hydroxyvitamin D and TPOAb titers in observational studies (Durá-Travé & Gallinas-Victoriano, 2024).
A randomized controlled trial published in the Indian Journal of Endocrinology and Metabolism enrolled 102 patients with newly diagnosed autoimmune thyroid disease, 93% of whom had vitamin D insufficiency. Patients who received cholecalciferol supplementation for 8 weeks experienced a 46.73% reduction in TPOAb titers compared to a 16.6% reduction in the control group. Sixty-eight percent of the supplemented group were classified as responders (at least 25% fall in TPOAb) versus 44% of controls (Chaudhary et al., 2016).
A 2024 meta-analysis found that vitamin D supplementation significantly decreased both TPOAb and TgAb titers in patients undergoing thyroid therapy. Supplementation at 1,500 to 2,000 IU per day for more than 12 weeks resulted in more significant decreases in TPOAb levels and greater increases in free T3 and free T4 compared to shorter durations (Shulhai et al., 2024).
A 2023 review specifically examining vitamin D’s immunopathological role in Hashimoto’s found that supplementation improved not only antibody titers but also cytokine markers including IP10, TNF-alpha, and IL-10, as well as the ratio of T-cell subsets Th17 and Tr1 (Lebiedziński & Lisowska, 2023).
The literature acknowledges that low vitamin D in Hashimoto’s patients may be partly a consequence of the disease itself, not only a cause. But the bidirectional relationship and the consistent evidence of benefit from supplementation in vitamin D-deficient patients supports regular monitoring in this population.
Ferritin: The Iron Connection Most Thyroid Patients Never Hear About
Iron deficiency and Hashimoto’s frequently coexist, and the relationship between them is bidirectional.
How iron affects thyroid hormone synthesis
Iron is the central atom in thyroid peroxidase (TPO), the hemoprotein enzyme responsible for thyroid hormone synthesis. Without adequate iron, TPO activity is impaired, and T4 and T3 production is reduced at the synthesis level. Iron also plays a role in T4-to-T3 conversion through its involvement in thyroxine deiodinase activity (Shulhai et al., 2024).
Several studies have found lower levels of free T3 and free T4 in individuals with iron deficiency, with hemoglobin and iron showing positive correlations with free T3 and free T4 but negative correlations with TSH (Shulhai et al., 2024).
Why Hashimoto’s patients are at higher risk
Many patients with Hashimoto’s have iron deficiency not just from dietary inadequacy but from comorbid autoimmune conditions. Autoimmune gastritis reduces iron absorption through its effect on gastric acid production. Celiac disease, which has a well-documented association with autoimmune thyroid disease, causes iron loss through intestinal inflammation. In a retrospective study, TSH, TPOAb, and anti-thyroglobulin antibody levels were significantly higher, while ferritin, hemoglobin, and serum iron were significantly lower, in 180 female patients with positive thyroid autoantibodies compared to 81 healthy controls (Shulhai et al., 2024).
As discussed in the ferritin blog in this series, standard lab ranges for ferritin in women are built from populations that likely included iron-deficient women, making the lower limit of normal structurally too low. Ferritin can also be artificially elevated by inflammation, which is chronically present in Hashimoto’s. A normal ferritin in the context of active thyroid autoimmunity deserves careful interpretation alongside a full iron panel including serum iron, TIBC, and transferrin saturation.
What a Functional Thyroid Workup Actually Looks At
A standard thyroid panel typically includes TSH and sometimes free T4. A more complete functional assessment includes:
TSH: pituitary signal, not a direct measure of thyroid output or tissue health
Free T4: storage form of thyroid hormone
Free T3: active thyroid hormone that drives cellular metabolism
Reverse T3: inactive T3 metabolite that can block T3 receptors; elevated in chronic stress, inflammation, and selenium deficiency
TPOAb: antibodies against thyroid peroxidase, the primary autoimmune marker in Hashimoto’s
TgAb: antibodies against thyroglobulin, elevated in a subset of Hashimoto’s patients
Selenium: assessed via serum selenium or selenoprotein P
Zinc: serum zinc or RBC zinc for a more functional assessment
25-hydroxyvitamin D: the standard measure of vitamin D status
Ferritin, serum iron, TIBC, transferrin saturation: full iron panel for functional iron assessment
CRP or inflammatory markers: essential context for interpreting ferritin in the presence of autoimmune activity
None of the nutrient markers in this list appear on a standard thyroid panel. Yet each of them directly affects how well your thyroid functions and how aggressively the autoimmune process progresses.
What This Means Clinically
Hashimoto’s is an autoimmune condition, not just a thyroid condition. Managing it effectively requires understanding the factors that drive immune dysregulation, thyroid hormone conversion, and oxidative stress, not just monitoring TSH.
Selenium, zinc, vitamin D, and ferritin are four of the most consistently documented nutrient gaps in this population. All four are assessable through blood work. All four have published evidence linking deficiency to worsened autoimmunity, impaired hormone production, or impaired T4-to-T3 conversion. And all four are frequently missed on standard panels.
The recommendation in functional practice is never to supplement based on diagnosis alone. It is to assess, identify what is actually low, and support the body with what it specifically needs.
If Your Labs Came Back Normal but You Still Feel This Way
This is exactly the kind of picture that gets missed when only TSH is checked. If you have Hashimoto’s, suspected thyroid dysfunction, or labs that have been called normal while your symptoms say otherwise, a Read Between the Labs session can help connect the dots.
It is a 30-minute telehealth review of your existing blood work with a written summary within 72 hours. No new testing required to get started.
To explore whether a deeper functional lab package is the right fit
References
Chaudhary, S., Dutta, D., Kumar, M., Saha, S., Mondal, S. A., Kumar, A., & Mukhopadhyay, S. (2016). Vitamin D supplementation reduces thyroid peroxidase antibody levels in patients with autoimmune thyroid disease: An open-labeled randomized controlled trial. Indian Journal of Endocrinology and Metabolism, 20(3), 391–398. https://doi.org/10.4103/2230-8210.179997
Durá-Travé, T., & Gallinas-Victoriano, F. (2024). Autoimmune thyroiditis and vitamin D. International Journal of Molecular Sciences, 25(6), 3154. https://doi.org/10.3390/ijms25063154
Kawai, M., Shoji, Y., Onuma, S., Etani, Y., & Ida, S. (2018). Thyroid hormone status in patients with severe selenium deficiency. Clinical Pediatric Endocrinology, 27(2), 67–74. https://doi.org/10.1297/cpe.27.67
Lebiedziński, F., & Lisowska, K. A. (2023). Impact of vitamin D on immunopathology of Hashimoto’s thyroiditis: From theory to practice. Nutrients, 15(14), 3174. https://doi.org/10.3390/nu15143174
Leone de Souza, L. S., Cassemiro, J. F., Campos, R. O., Rende, P. R. F., Braga Filho, J. S., Hecht, F., dos Santos de Jesus, J., Anuncição, S. M., & Ramos, H. E. (2025). Selenium nutritional status and thyroid dysfunction. Archives of Endocrinology and Metabolism, 69(1), e230348. https://doi.org/10.20945/2359-4292-2023-0348
Rabbani, E., Golgiri, F., Janani, L., Moradi, N., Fallah, S., Abiri, B., & Vafa, M. (2021). Randomized study of the effects of zinc, vitamin A, and magnesium co-supplementation on thyroid function, oxidative stress, and hs-CRP in patients with hypothyroidism. Biological Trace Element Research, 199(11), 4090–4101. https://doi.org/10.1007/s12011-020-02548-3
Shulhai, A.-M., Rotondo, R., Petraroli, M., Patianna, V., Predieri, B., Iughetti, L., Esposito, S., & Street, M. E. (2024). The role of nutrition on thyroid function. Nutrients, 16(15), 2496. https://doi.org/10.3390/nu16152496