
What an Organic Acids Test Reveals That Standard Blood Work Misses
Your blood work came back normal. Your doctor says everything looks fine. And yet you are exhausted, your mood is unstable, your digestion feels off, and nothing you try seems to move the needle. Standard blood work is designed to rule out acute disease. It is not designed to assess the functional state of your metabolism, your nutrient status at the cellular level, or what your gut microbiome is producing. That is a different question. And it requires a different test.
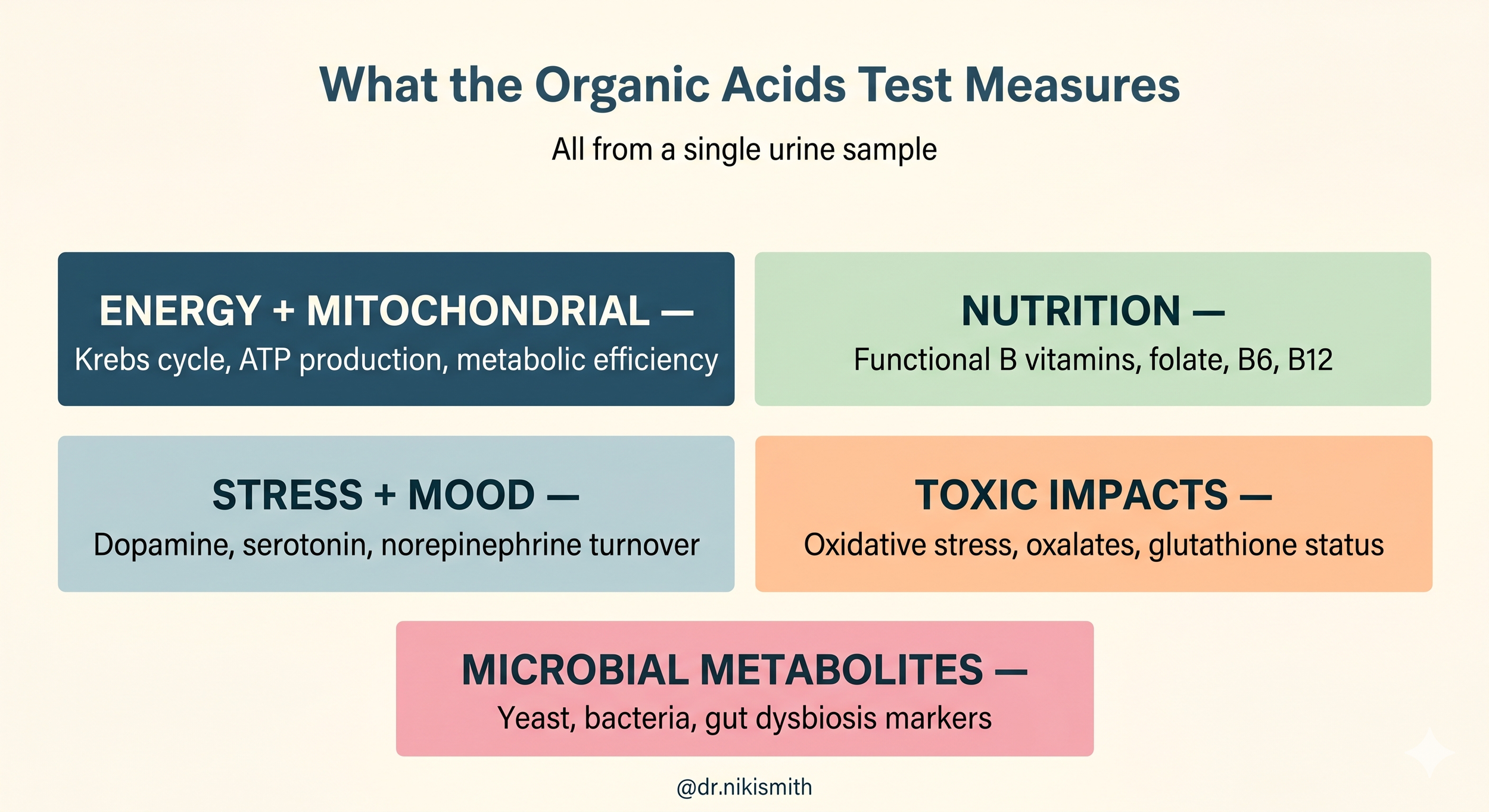
The organic acids test, or OAT, is a urine-based assessment that measures metabolic byproducts from the body's core biochemical pathways. When these pathways are running well, metabolic intermediates flow smoothly and organic acid levels stay within expected ranges. When pathways are blocked, whether due to nutrient insufficiency, mitochondrial dysfunction, gut dysbiosis, or toxic burden, organic acids accumulate and spill into the urine. The pattern tells a story that serum markers alone cannot tell (Diagnostic Solutions Laboratory, 2024; Kansakar et al., 2017).
This post covers the five major sections of the OAT and what each reveals clinically, with a focus on the markers most relevant for women with ADHD, PMDD, fatigue, and hormonal symptoms.
What Organic Acids Are and Why They Matter
Organic acids are small molecules produced as byproducts of normal metabolic reactions. They are intermediate metabolites of critical pathways including the Krebs cycle, fatty acid metabolism, amino acid catabolism, neurotransmitter synthesis, and microbial activity (Kansakar et al., 2017).
A targeted metabolomics analysis of 22 organic acids in 122 healthy adults found that urine organic acids reflect the activity of main metabolic pathways and can be used to assess health status, nutritional status, vitamin deficiencies, and response to environmental factors.

The study confirmed that organic acid quantification in urine provides a valid and sensitive approach to evaluating metabolic function in a clinical setting (Kansakar et al., 2017).
Unlike standard serum labs, which measure circulating levels at a single point in time, the OAT captures what is actually happening inside cells and in the gut, reflecting metabolic activity across a broader physiological window. It is collected as a first morning urine sample after an overnight fast, which provides the most representative snapshot of baseline metabolic activity (Diagnostic Solutions Laboratory, 2024).
Section One:
Energy and Mitochondrial Function
The first and often most clinically telling section of the OAT assesses how well your mitochondria are producing energy. Mitochondria convert dietary macronutrients into ATP through glycolysis, the Krebs cycle, and oxidative phosphorylation. When this process is impaired, Krebs cycle intermediates accumulate in urine.
What the Krebs cycle markers show
Markers including citric acid, cis-aconitic acid, isocitric acid, alpha-ketoglutaric acid, succinic acid, fumaric acid, and malic acid represent sequential steps in the Krebs cycle. Elevation or depletion of specific markers can identify exactly where the cycle is congested or blocked, and which nutrient cofactors are insufficient.
Every step of the Krebs cycle requires specific B vitamins and minerals as cofactors. Thiamine (B1), riboflavin (B2), niacin (B3), pantothenic acid (B5), lipoic acid, magnesium, and CoQ10 are among the primary cofactors. When any of these are insufficient, the corresponding step slows down, upstream intermediates accumulate, and the pattern appears in urine organic acids (Diagnostic Solutions Laboratory, 2024).
Succinic acid elevation, for example, is a strong indicator of mitochondrial dysfunction and is associated with impaired iron-sulfur cluster dependent enzyme activity. Iron deficiency can directly decrease succinate dehydrogenase function (Diagnostic Solutions Laboratory, 2024).
Lactate, pyruvate, and mitochondrial stress
Elevated lactate and pyruvate on the OAT indicate a shift toward anaerobic metabolism, meaning cells are not efficiently converting pyruvate into energy through the Krebs cycle. This pattern is associated with B1 deficiency, CoQ10 insufficiency, and mitochondrial stress.
A comprehensive review of mitochondrial biomarkers confirmed that lactate and the lactate:pyruvate ratio remain among the most established indicators of mitochondrial dysfunction, particularly when elevated together. Pyruvate elevation is strongly associated with thiamine (B1) deficiency, which is required for pyruvate dehydrogenase activity (Shayota, 2023).
For women with ADHD, PMDD, or chronic fatigue, mitochondrial dysfunction is a clinically underrecognized driver. The brain is one of the most metabolically demanding organs in the body. When mitochondrial energy production is impaired, cognitive function, mood regulation, and executive function are among the first things to decline.

Section Two:
Nutritional Status and Functional B Vitamin Deficiency
One of the most valuable clinical applications of the OAT is its ability to identify functional vitamin deficiencies even when serum levels look normal. This distinction, between circulating levels and actual cellular function, is one of the most important gaps in standard lab interpretation.
Methylmalonic acid and functional B12 deficiency
Methylmalonic acid (MMA) accumulates in urine when vitamin B12 is insufficient. Vitamin B12 is required for the enzyme that converts MMA to succinyl-CoA. When B12 is low at the functional level, MMA backs up and spills into urine. Importantly, serum B12 can appear normal while MMA is elevated, because serum B12 measures circulating levels, not functional cellular availability (Diagnostic Solutions Laboratory, 2024).
Common drivers of functional B12 insufficiency that standard testing misses include low stomach acid, gut dysbiosis, metformin use, proton pump inhibitor use, and impaired absorption from conditions like celiac disease or atrophic gastritis.
FIGLU and functional folate deficiency
Formiminoglutamic acid (FIGLU) is an intermediate metabolite in the pathway that converts histidine to glutamic acid. Folate is required for this conversion. When folate is functionally insufficient, FIGLU accumulates and appears in urine.
A study of patients with formiminoglutamic aciduria, a condition of impaired folate metabolism, confirmed that FIGLU elevation reliably identifies functional folate insufficiency even in cases where serum folate appears within normal limits. The severity of FIGLU elevation correlated with the degree of functional folate pathway impairment (Ahrens-Nicklas et al., 2019).
Folate is required upstream for serotonin and dopamine synthesis. For women with PMDD or ADHD, functional folate deficiency may be contributing to neurotransmitter instability in ways that standard serum folate levels would completely miss.
Xanthurenate and functional B6 deficiency
Xanthurenic acid is a metabolite produced when tryptophan is broken down through the kynurenine pathway. This pathway requires vitamin B6 as a cofactor at multiple steps. When B6 is functionally insufficient, kynurenine accumulates and is shunted toward xanthurenic acid, which then appears elevated in urine.
Xanthurenic acid elevation is considered one of the earliest and most sensitive functional markers of B6 insufficiency. A classic demonstration of this mechanism involved two children with mental retardation who showed markedly elevated xanthurenate and related kynurenine metabolites in urine following tryptophan loading, despite normal serum pyridoxal phosphate levels. Treatment with high-dose B6 temporarily normalized the pattern, confirming that xanthurenate elevation can reflect a functional B6 dependency even when serum levels appear adequate (Tada et al., 1967).
More recent work has confirmed that ratios of kynurenine pathway metabolites, including the hydroxykynurenine to xanthurenate ratio, correlate more strongly with functional B6 status than individual metabolite levels alone, and normalize after B6 supplementation is initiated (Ciorba, 2013).
B6 is a required cofactor for serotonin, dopamine, and GABA synthesis. Functional B6 deficiency is one of the more clinically meaningful findings on an OAT in women with mood instability, PMDD, and ADHD, and it is one of the more correctable.
Section Three:
Stress, Mood, and Neurotransmitter Metabolism
The stress and mood section of the OAT measures urinary metabolites that reflect the turnover of dopamine, norepinephrine, epinephrine, and serotonin. These are not direct measurements of neurotransmitter levels. They are downstream metabolites that indicate how actively these neurotransmitters are being produced and broken down.
Homovanillic acid: dopamine turnover
Homovanillic acid (HVA) is the major urinary metabolite of dopamine. It represents dopamine turnover and is produced through the combined activity of monoamine oxidase (MAO) and catechol-O-methyltransferase (COMT). Very low HVA on the OAT may indicate reduced dopamine turnover or impaired dopamine synthesis, and is associated with higher scores on depression assessments. Elevated HVA reflects increased dopamine activity, which can be seen in chronic stress and anxiety states (Diagnostic Solutions Laboratory, 2024).
Importantly, HVA is also a metabolite of microbial bioactivity on dietary flavonoids. Elevated HVA should prompt a review of gut dysbiosis markers on the same panel.
Vanillylmandelic acid: norepinephrine and epinephrine turnover
Vanillylmandelic acid (VMA) reflects the turnover of epinephrine and norepinephrine. Chronically elevated VMA is associated with sustained stress response activation, PTSD, and anxiety states. The HVA to VMA ratio provides additional clinical information, reflecting the balance between dopamine and norepinephrine metabolism and the activity of dopamine-beta-hydroxylase (DBH), the enzyme that converts dopamine to norepinephrine (Diagnostic Solutions Laboratory, 2024).
For women with ADHD, where dopamine and norepinephrine regulation are central to the symptom picture, these markers offer a functional window into neurotransmitter activity that no standard blood panel provides.
5-HIAA: serotonin turnover
5-Hydroxyindoleacetic acid (5-HIAA) is the primary urinary metabolite of serotonin. Low 5-HIAA indicates reduced serotonin production or turnover and is associated with depression and anxiety. Elevated 5-HIAA can be seen in those taking SSRIs or 5-HTP supplements and should be interpreted in that context (Diagnostic Solutions Laboratory, 2024).
Only one to two percent of tryptophan is metabolized through the serotonin pathway. The majority flows through the kynurenine pathway. The balance between these two routes is influenced by inflammation, B6 status, and gut microbial activity, all of which can be assessed simultaneously on the OAT.
Quinolinic acid: the neuroinflammatory marker
Quinolinic acid is produced through the kynurenine pathway and acts as an NMDA receptor agonist. At elevated levels it is considered excitotoxic and neuroinflammatory. Elevated quinolinic acid has been associated with autism spectrum disorder, suicidal ideation, viral infections, and metabolic syndrome. Its ratio to kynurenic acid, which is neuroprotective, provides a measure of the balance between neuroinflammatory and neuroprotective states (Diagnostic Solutions Laboratory, 2024).
Section Four:
Toxic Impacts and Oxidative Stress
The toxic impacts section assesses oxidative stress, toxic exposures, glutathione status, and oxalate metabolism. For women with ADHD and PMDD, oxidative stress and impaired antioxidant defense are clinically relevant and often overlooked.
Oxalate: more than kidney stones
Oxalic acid on the OAT reflects both dietary oxalate intake and endogenous oxalate production. Elevated oxalate is associated with kidney disease, cardiovascular conditions, cellular inflammation, and mitochondrial toxicity. Endogenous oxalate production is primarily hepatic and is influenced by glycine availability, vitamin C intake, and gut microbial activity.
Oxalobacter formigenes, a gut bacteria, is the primary microbial degrader of oxalate. When gut dysbiosis reduces Oxalobacter populations, oxalate absorption increases. Vitamin B6 supplementation may reduce oxalate production by supporting the enzymatic conversion of glyoxylate away from oxalic acid (Diagnostic Solutions Laboratory, 2024).
Glutathione markers
Alpha-hydroxybutyric acid and pyroglutamic acid on the OAT reflect glutathione synthesis and demand. Elevated alpha-hydroxybutyric acid indicates increased glutathione production, suggesting the body is under oxidative stress. Elevated pyroglutamic acid reflects impaired glutathione recycling due to cysteine or glycine insufficiency (Diagnostic Solutions Laboratory, 2024).
Glutathione is the primary endogenous antioxidant. In neurodivergent populations and in women under chronic hormonal and metabolic stress, glutathione demand is often elevated while the building blocks needed to produce it are frequently depleted.
Section Five: Microbial Metabolites
The microbial metabolites section is one of the most clinically distinctive features of the OAT. It captures urinary byproducts of gut microbial activity, providing indirect evidence of dysbiosis, yeast overgrowth, and bacterial imbalance without requiring a stool sample.
Arabinitol: a marker of Candida activity
Arabinitol is a five-carbon sugar alcohol produced by most pathogenic Candida species. Elevated urinary arabinitol is a sensitive indicator of Candida overgrowth or invasive candidiasis. Research using gas chromatography-mass spectrometry demonstrated that the D-arabinitol to L-arabinitol ratio is elevated in patients with confirmed invasive candidiasis and normalizes during effective antifungal treatment (Christensson et al., 1999). A subsequent prospective study in neonatal intensive care patients confirmed that elevated urine D-arabinitol ratios reliably identified invasive candidiasis, in some cases several days before blood cultures turned positive (Sigmundsdottir et al., 2000).
In the functional medicine context, arabinitol elevation on the OAT suggests gut yeast overgrowth. This is clinically relevant because Candida overgrowth is associated with impaired nutrient absorption, increased intestinal permeability, and systemic inflammatory burden.
3,4-DHPPA: a microbial metabolite of dietary polyphenols
3,4-Dihydroxyphenylpropionic acid (3,4-DHPPA) is produced primarily by the microbial action of Clostridium species, Escherichia coli, Bifidobacterium, Lactobacillus, and Eubacterium on dietary polyphenols, as well as on dopamine and aromatic amino acids. It has documented antioxidant properties and has been shown to significantly inhibit the secretion of pro-inflammatory cytokines from macrophages (Li et al., 2022).
Low 3,4-DHPPA on the OAT is associated with insufficient polyphenol intake or reduced levels of the beneficial bacteria that produce it. Its elevation correlates with higher homovanillic acid, reflecting the connection between gut microbial activity and dopamine metabolism (Diagnostic Solutions Laboratory, 2024).
Clostridia metabolites and neurotransmitter disruption
Several Clostridium species produce metabolites that directly affect neurotransmitter pathways. Clostridium difficile and related species have been associated with alterations in gut microbiota composition that affect tryptophan availability, serotonin production, and systemic inflammatory tone. Research on gut microbiota and Clostridium difficile has confirmed that dysbiosis involving Clostridium overgrowth disrupts the balance of the gut microbial community in ways that have measurable downstream effects on host health and immune regulation (Piccioni et al., 2022).
On the OAT, patterns consistent with Clostridia overgrowth include elevated 4-hydroxyphenylacetic acid, elevated phenylacetic acid, and disrupted tryptophan metabolite patterns. These microbial markers do not replace a GI-MAP, but they provide a biochemical snapshot of what the gut is producing systemically.
What the OAT Shows That Blood Work Cannot
To make this concrete: a woman with ADHD, PMDD, fatigue, and mood instability might have a completely normal comprehensive metabolic panel, normal CBC, and normal thyroid panel. A standard workup would find nothing actionable.
An OAT on the same patient might reveal:
Elevated succinic acid indicating mitochondrial dysfunction at the Krebs cycle level
Elevated methylmalonic acid showing functional B12 deficiency despite normal serum B12
Elevated xanthurenate confirming functional B6 insufficiency affecting serotonin and dopamine synthesis
Elevated FIGLU showing folate pathway impairment that is not captured by serum folate
Low HVA and low 5-HIAA suggesting reduced dopamine and serotonin turnover
Elevated arabinitol indicating gut yeast overgrowth contributing to systemic inflammation
Elevated quinolinic acid reflecting neuroinflammatory burden in the kynurenine pathway
None of these would appear on a standard metabolic panel. All of them are clinically addressable. And all of them are documented causes or amplifiers of the symptoms she came in with.
This is what functional testing is designed to do. Not find exotic diseases. Ask more precise questions about what is actually happening in the systems that drive daily function.
Want to Know What Your Metabolic Picture Actually Looks Like?
The OAT is included in the 3-Month Functional Lab Package at Botanical Health Clinic alongside a GI-MAP and comprehensive blood chemistry. Together these tests build a complete functional picture of what is driving your symptoms from the ground up.
If you are curious whether this level of investigation is the right next step for you, a free discovery call is the best place to start.
References
Ahrens-Nicklas, R. C., Ganetzky, R. D., Rush, P. W., Conway, R. L., & Ficicioglu, C. (2019). Characteristics and outcomes of patients with formiminoglutamic aciduria detected through newborn screening. JIMD Reports, 48(1), 63–70. https://doi.org/10.1002/jmd2.12049
Christensson, B., Sigmundsdottir, G., & Larsson, L. (1999). D-arabinitol: A marker for invasive candidiasis. Medical Mycology, 37(6), 391–396. https://doi.org/10.1080/02681219980000601
Ciorba, M. A. (2013). Kynurenine pathway metabolites: Relevant to vitamin B-6 deficiency and beyond. The American Journal of Clinical Nutrition, 98(4), 834–835. https://doi.org/10.3945/ajcn.113.072215
Diagnostic Solutions Laboratory. (2024). OAp – Organic Acids Profile: Interpretive guide. https://www.diagnosticsolutionslab.com/assets/documents/oap-organic-acids-interpretive-guide.pdf
Kansakar, U., Trimarco, V., Mone, P., Varzideh, F., Lombardi, A., & Santulli, G. (2017). Application of metabolomics: Focus on the quantification of organic acids in healthy adults. International Journal of Molecular Medicine, 40(1), 112–120. https://doi.org/10.3892/ijmm.2017.3012
Li, R., Xie, L., Li, L., Chen, X., Yao, T., Tian, Y., Li, Q., Wang, K., Huang, C., Li, C., Li, Y., Zhou, H., Kaplowitz, N., Jiang, Y., & Chen, P. (2022). The gut microbial metabolite, 3,4-dihydroxyphenylpropionic acid, alleviates hepatic ischemia/reperfusion injury via mitigation of macrophage pro-inflammatory activity in mice. Acta Pharmaceutica Sinica B, 12(4), 1790–1803. https://doi.org/10.1016/j.apsb.2021.05.029
Piccioni, A., Rosa, F., Manca, F., Pignataro, G., Zanza, C., Savioli, G., Covino, M., Ojetti, V., Gasbarrini, A., Franceschi, F., & Candelli, M. (2022). Gut microbiota and Clostridium difficile: What we know and the new frontiers. International Journal of Molecular Sciences, 23(21), 13323. https://doi.org/10.3390/ijms232113323
Shayota, B. J. (2023). Biomarkers of mitochondrial disorders. Mitochondrion, 73, 83–94. https://doi.org/10.1016/j.mito.2023.10.003
Sigmundsdottir, G., Christensson, B., Bjorklund, L. J., Håkansson, K., Pehrson, C., & Larsson, L. (2000). Urine D-arabinitol/L-arabinitol ratio in diagnosis of invasive candidiasis in newborn infants. Journal of Clinical Microbiology, 38(8), 3039–3042. https://doi.org/10.1128/JCM.38.8.3039-3042.2000
Tada, K., Yokoyama, Y., Nakagawa, H., Yoshida, T., & Arakawa, T. (1967). Vitamin B6 dependent xanthurenic aciduria. Tohoku Journal of Experimental Medicine, 93(2), 115–124. https://doi.org/10.1620/tjem.93.115